This One Fix Could Prevent 50,000 Suicide Deaths
Erik Messamore, MD, PhD
A Suicide Prevention Proposal
Today is Suicide Prevention Awareness Day.
As a psychiatric physician—and simply as someone who cares about other people—I join millions of other voices hoping to move our society closer to one that can better prevent suicide.
Preventing suicide is easier said than done. It’s not an easy task for a front-line doctor. It can be even harder for a government, or mental health agency, or insurance company to devise effective policies that can reduce suicide.
But there is one administrative or policy action that governments, agencies, or insurers could make that is guaranteed to reduce suicide rates.
That policy action?
Encourage and support clinics and clinicians to prescribe clozapine.
Let Me Introduce You to Clozapine
I was once working at a state hospital and became the doctor for a lady with schizophrenia. Let’s call her “Anna.” She had been continuously ill for about 20 years, bouncing between the hospital, the street, and sometimes the jail. As a homeless person with severe mental illness, she had experienced many really horrible traumas.
Anna had never tried clozapine because: 1) doctors assumed that she would not take the medication regularly, or that her “lifestyle” was too chaotic to be able to show up for the FDA-required weekly blood tests; and 2) she was very afraid of needles so would refuse the offer of clozapine anyway.
To address her fear of needles, I prescribed an anesthetic cream that we would rub into the spot where we would draw blood. The anesthetic cream to numb the skin helped Anna feel comfortable with blood testing and she agreed to try clozapine.
Within two months, we saw the real Anna. She was a delightful lady with a quick wit and wry sense of humor. And she became able, for the first time since becoming ill, to actively participate in her discharge planning.
She took her medication regularly because she felt that it really helped her. (Like most anyone else would do, the reason she would stop taking her prior medications is because they were not really helping in ways that mattered to her.)
She went on to get her own apartment and began to create the kind of life she wanted. Clozapine helped her break the cycle of illness and homelessness and allowed Anna to reclaim a life in which she was in charge
Clozapine is, without a doubt, the world’s most effective treatment for the most difficult forms of schizophrenia.
How Many People With Schizophrenia Should Be Using Clozapine?
At least 15% of people with schizophrenia should be receiving clozapine. This figure is based on widely-accepted findings that:
1) the type of schizophrenia for which clozapine is appropriate (the poorly-named ‘treatment-resistant’ type) comprises at least 30% of people with schizophrenia; and
2) clozapine is effective in at least half of people who take it.
Based on real world data from other countries, this 15% estimate is probably on the low side. In most countries throughout Europe, Oceana, and Asia between 15% to 30% of people with schizophrenia are offered the unique benefits of clozapine.
In the United States, that figure is 4%.
Not only should this embarrass the bejeebers out of Americans, it’s also a humanitarian disaster.
Let’s Do The Clozapine Math
Schizophrenia affects about 1 of every 100 people. That means that there are about 3.3 million people in the USA with schizophrenia.
Of that 3.3 million people, some 30% will have the kind of schizophrenia for which clozapine is the best option. That’s over 1 million people whose illness won’t get better with the usual schizophrenia treatments.
If we want to be on par with the practice of other developed countries, some 20% of people with schizophrenia should receiving clozapine. For the US, that would be 654,000 people.
In reality, only 4% of people with schizophrenia in the United States are being offered clozapine (130,800 people).
So the American clozapine gap—the difference between number of people who should be seeing the benefits of clozapine versus the number who actually get it—is 523,200.
That’s more than the number of people living in Atlanta, Georgia.
Now, The Suicide Math
We should not think of this clozapine gap as some regrettable quirk of healthcare policy. Clozapine is the only medication that has FDA approval to reduce the risk of suicide in schizophrenia-spectrum illnesses. So the American clozapine gap translates directly into suicides that we could prevent… but don’t.
The math:
About 50% of people with schizophrenia will attempt suicide during the course of their illness.
About 10% of people with schizophrenia will die from suicide.
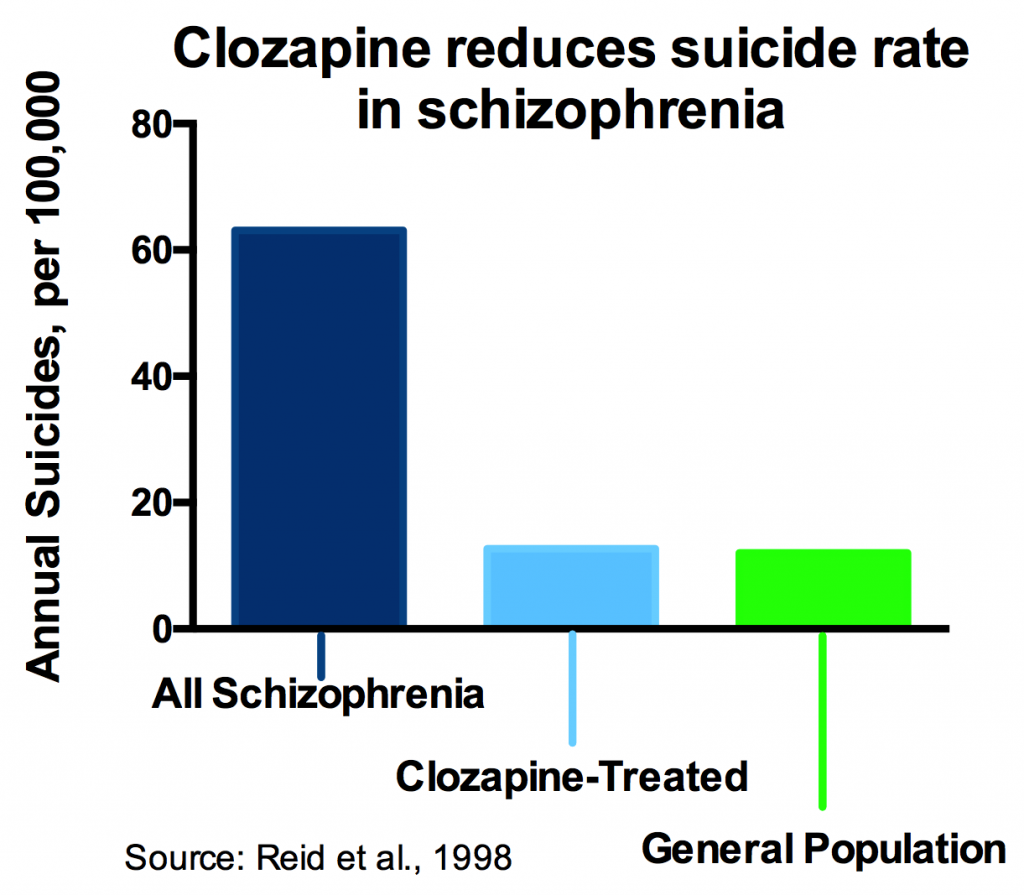
Meanwhile, some studies have shown that suicide rates in schizophrenia plummet to the population baseline rate when people are treated with clozapine.
With 500,000 people with schizophrenia who would get better with clozapine but are not offered it and a 10% rate of suicide mortality, that’s a half million lives at risk and up to 50,000 deaths from suicide that we could prevent—but politically, economically, and logistically—choose not to.
Let’s Think About the Lost Opportunities
This glaring deficiency of the American medical system also means that a half-million people with an easily-treatable illness are denied the opportunity to complete their education, return to work, grow their social support network, realize their full human potential.
Instead these neglected souls are destined to cycle between hospitals, jails, crappy nursing facilities, or the street.
Please… think about that for a while. Then tell others about it.
Let’s Save 500,000 Lives
Every other developed country on planet earth has managed to figure out how to get clozapine into the hands of the people who need it. It’s time we do the same.
If you are a government official, public health influencer, mental health clinic decision maker, or insurance company executive who wants to make a serious dent into the suicide problem, let’s get together and make it easier for people who need clozapine to get it.
And if you’re not a policy-maker, you can call, post, tweet and insist that your government, insurance company, or local clinic solve the clozapine access problem.
Not only will we prevent about 50,000 suicides, we will improve the lives of the 500,000 people caught in America’s clozapine gap, and the several million lives of their families and friends. And if we can move someone from homeless to housed, or hospitalized to employed, we all benefit from closing the clozapine gap.
Let’s Learn About Clozapine
If you are a prescribing clinician who cares for people with schizophrenia and want to learn more about how to use this unique and life-saving medication, the NEOMED Clozapine Assistance Service offers free quarterly trainings. Look here for information about the training schedule.
Disclaimers
This article summarizes the results and conclusions of articles published in the medical literature. It is for general information. It is not a substitute for medical advice, and readers are admonished not to enact or change treatments based on this article. Always seek the advice of your doctor before starting or changing treatment.
The thoughts, views, and opinions expressed in this article are my own and do not reflect or represent the policy or position of Northeast Ohio Medical University